













Keeping pace
Life-changing advances and a multidisciplinary approach give new hope to patients with Merkel cell carcinoma
Feature
By Allison Evans, Assistant Managing Editor, November 1, 2021

When Paul Nghiem, MD, PhD, FAAD, first started treating patients with skin cancer almost 20 years ago, physicians had little understanding of how to treat their patients with Merkel cell carcinoma (MCC). “Everybody knows it’s aggressive, but it’s about 40% likely to recur, which is a much higher number than any other skin cancer, and that’s after totally optimal care.”
If a patient is in the lowest risk category, the chance of recurrence is still above 10%, said Dr. Nghiem, head of dermatology at University of Washington School of Medicine, and director of the Skin Oncology Clinical Program at the Seattle Cancer Care Alliance. A multidisciplinary approach is critical in caring for patients with MCC, he stated. “Merkel cell carcinoma is a tricky cancer, and each specialty feels that they can attack it with their tools — but they may not have all the tools they need.”
Oftentimes, MCC is diagnosed in a dermatologist’s office with a skin biopsy, said Song Y. Park, MD, IFAAD, a dermatologist at the Seattle Cancer Care Alliance and acting instructor in the Division of Dermatology at the University of Washington School of Medicine. “While the initial diagnosis can be intimidating to both physician and patient, dermatologists can help patients by guiding appropriate initial work-up and referral. Also, as the patient will likely need lifelong skin surveillance, dermatologists can assist with optimal surveillance of MCC and other skin cancers.”
This month, experts discuss the latest advances in the management and treatment of MCC, as well as the critical role dermatologists play in the care team for MCC patients.
Merkel cell polyomavirus – consider quantification of MCPyV oncoprotein antibodies at baseline
In 2008, researchers first identified what became known as Merkel cell polyomavirus (MCPyV), a small tumor virus, similar to human papillomaviruses, in MCC tumor tissues. Close to 80% of MCC cases in the United States are driven by infection with MCPyV, while the remaining 20% of cases are caused by UV radiation-induced damage. While about 50% of individuals in the United States are infected during childhood, the virus must develop two unlikely mutations to become oncogenic.
“While the presence of MCPyV doesn’t change treatment options for MCC patients, it is an important prognostic factor for determining a surveillance strategy,” Dr. Park said.
“About half of all newly diagnosed MCC patients produce antibodies to the MCPyV oncoprotein. Such sero-positive patients have a 42% decrease in the risk of recurrence, and the antibody titer can be used to detect early disease recurrence. Sero-negative patients need to be followed with scans,” Dr. Nghiem said.
MCC patients with strong immune responses to the virus have better disease outcomes, providing a strong rationale for the application of immunotherapy (J Natl Compr Canc Netw. 2018 Jun;16(3):782-90).
Baseline scans – consider as part of staging for most patients
The National Cancer Care Network® (NCCN) released updated MCC guidelines in February 2021, Dr. Nghiem said. (Download the guidelines). “A PET-CT scan is indicated in most patients with MCC, very unlike melanoma or any other skin cancer. The baseline PET is more than twice as sensitive as a baseline CT scan,” Dr. Nghiem said.
“A PET-CT scan is indicated in most patients with MCC, very unlike melanoma or any other skin cancer. The baseline PET-CT is more than twice as sensitive as a baseline CT scan.”
“Even for small, low-risk primary lesions with no nodal involvement, there is a significant risk of occult metastatic disease such that across all newly diagnosed Merkel patients, about one in six will have occult nodal or distant disease found on a PET-CT scan that massively changes management for those patients,” he explained.
Surgical margins and radiation
One of the more important developments in the management of MCC is the understanding of how to integrate surgery and radiation, Dr. Nghiem said. Previous studies have shown that wider surgical margins are associated with improved local control of MCC. However, most of these studies did not track whether the patient also received adjuvant radiotherapy, which greatly affects local recurrence risk, he explained.
“We need to shift ‘wide margins’ to ‘wise margins,’” Dr. Nghiem said. “This means you don’t blindly take a huge margin in every case, but you plan out what the risk factors are, what the location is, and whether or not you are giving radiation.”
In a JAAD study that Dr. Nghiem was also a co-author on, they found that if adjuvant radiotherapy is given, patients with narrow or even microscopically positive margins have excellent local disease control. If adjuvant radiotherapy is planned, narrower surgical margins are adequate, reduce morbidity, and minimize delay in initiating radiotherapy (2021 Feb;84(2):340-7).
“If you’re going to radiate anyway, you don’t need a huge margin. If you do take a large margin, and especially if you move a lot of tissue or have a complicated graft, then you must delay radiation sometimes by months,” he explained.
When to radiate
“I like to take the tumor out surgically before radiation, if possible,” Dr. Nghiem said. “But in Australia, they typically just radiate the cancer, and surgery is done after the biopsy. I think you get better outcomes with at least a modest excision to get the gross clinical tumor out and follow it with radiation, if needed.”
There are six factors that most centers use to determine whether to consider giving radiation, Dr. Nghiem explained. “If a patient is negative in all six factors, most physicians would not advocate radiating such a low-risk lesion. If, however, patients have one or more risk factor, then physicians need to balance the risks and benefits of radiation. The six factors are: negative pathologic margins, no lymphovascular invasion, primary smaller than 2 cm, primary NOT on the head/neck, no systemic immune suppression, and negative sentinel lymph node biopsy.”
“At the time you send a patient for re-excision and probable sentinel lymph node biopsy (because most patients probably would benefit from a sentinel lymph node biopsy), you’re still missing two pieces of information: You don’t know what the sentinel lymph node biopsy result will be, and you don’t know what your pathologic margins will be. Do you have margin-positive disease, or did you get it all by a large margin?” Dr. Nghiem said.
“You do know, however, whether the patient is immune suppressed, how big the tumor is, whether there is gross clinical disease or not, and if there is lymphovascular invasion. Those are some relevant factors to determine whether you need radiation to clean up or not,” he said.
“If a patient has several of those factors up front, then the patient is clearly high risk and you know you’re going to need to radiate — which means you don’t need to be aggressive surgically because the radiation is fantastic at cleaning up microscopic or even grossly positive margins,” Dr. Nghiem said (see figure 3 in JAAD).
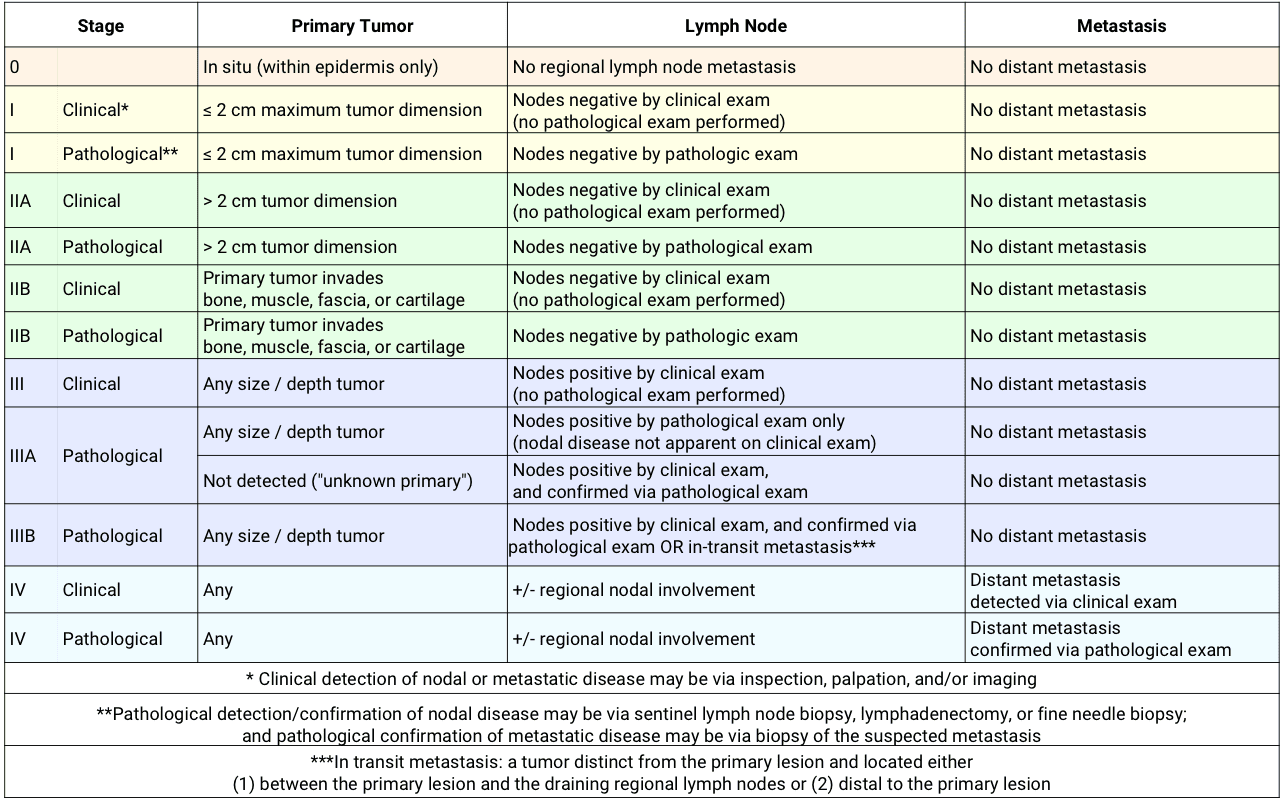
The AJCC MCC staging criteria
The first consensus Merkel carcinoma staging system was published in 2010. In January 2018, the AJCC 8th edition staging system replaced the 7th edition staging system, which included two important differences.
First, when the stage is determined, physicians should designate whether it was determined ‘clinically’ or ‘pathologically,’ as this has implications in recurrence and survival. Clinical stages can be determined by inspection, palpation of the lymph nodes, or imaging studies. Pathological stages are based on results of sentinel lymph node biopsy, lymphadenectomy, or fine needle biopsy.
Second, “one of the most significant changes to the 8th edition of AJCC staging for Merkel cell carcinoma is the regrouping and downstaging of patients who have clinically detectable lymph node metastasis and an unknown primary site from stage IIIB to stage IIIA,” said Kelly Harms, MD, PhD, FAAD, associate professor of dermatology at the University of Michigan, chief of the Division of Cutaneous Surgery and Oncology, and director of the Multidisciplinary Cutaneous Oncology Program at Michigan Medicine.
Many studies have shown that node-positive patients with an unknown primary tumor have an improved survival outcome compared to node-positive patients who have a visible tumor. “We found that when patients have a clinically detectable regional metastasis but lack a clinically identifiable primary tumor, their prognosis was more similar to patients whose metastases were microscopically detectable (stage IIIA) rather than clinically detectable (stage IIIB). This prompted us to reclassify patients with MCC of unknown primary as stage IIIA,” Dr. Harms said.
Some studies suggest that since the immune system eliminated the primary tumor in the ‘unknown primary’ cases, the immune system is better able to eliminate other microscopic disease that may have spread elsewhere.
View the 8th edition staging system chart. A list of major referral centers is available.
Surveillance
The Merkel recurrence risk goes down faster after diagnosis than most cancers, Dr. Nghiem explained. “Ninety percent of recurrences will happen within three years. After three years you can — and should — calm down your surveillance. A good number of Merkels will recur where you can’t find them clinically, so you’ll want to be doing scans or blood tests, depending on what the situation is,” he said.
Performing an oncoprotein antibody (AMERK) test at baseline is useful for all MCC patients. “This is because patients who do not produce oncoprotein antibodies are at higher risk of having a recurrence and need to be followed closely by imaging scans. In contrast, patients who produce oncoprotein antibodies can be followed over time using this test which decreases the need for imaging scans, and can help discover recurrences when they are small,” Dr. Nghiem said.
“If a patient’s tumor is positive for polyomavirus and they make those antibodies at diagnosis, then the antibodies will go down if the cancer does not recur, and they will go up over time if the cancer starts to recur. Antibody production is very, very sensitive for disease recurrence,” he said.
Dr. Nghiem has worked to create and maintain the website MerkelCell.org for nearly 20 years, which has a beta version of an MCC recurrence risk calculator that plots out where the patient is in their post-diagnosis journey. “This risk calculator includes validated risk factors that aren’t included in MCC staging, including sex, immune suppression, and age. If a patient gets their risk of recurrence down to less than 2%, the physician likely does not need to perform significant surveillance anymore,” he said.
Another test being investigated is a circulating tumor DNA (ctDNA) test that can work especially well for virus-negative patients, Dr. Nghiem said. “Many of us are looking into how well this test will work for MCC patients.”
“We are currently investigating the sensitivity and specificity of this test because theoretically ctDNA should identify minimal residual disease. We already know that it can detect 0.6 cm of disease — that’s less than you can detect on a PET scan,” said Lisa Zaba, MD, PhD, FAAD, clinical associate professor of dermatology at Stanford School of Medicine and director of the Stanford multi-disciplinary Merkel Cell Carcinoma Clinic at the Stanford Cancer Center. “We are looking at this test as something that could detect residual tumor for both MCPyV-positive and MCPyV-negative patients and help guide physicians on which stage III patients may need adjuvant therapy to prevent recurrence.”
Each cancer has a very different relationship to ctDNA, Dr. Zaba said. “Scientists have been trying to use ctDNA for melanoma and is hasn’t worked well. But it seems like Merkel cell may be one of the most appropriate cancers for this test. The hope is that dermatologists should be able to access ctDNA testing in about a year.”
Before immune checkpoint inhibitors
Before the approval of immune checkpoint inhibitors (ICI) for advanced MCC, chemotherapy was a standard treatment that provided a short-lived response of about 90 days. Within nine months after starting chemotherapy, more than 90% of patients have tumor progression, Dr. Park noted. “PD-1/PD-L1 inhibitors, however, have shown about a 50-70% overall response, with a majority of the responses being durable.”
“A common misconception about MCC treatments surrounds the use of platinum-based chemotherapies as first- or second-line treatments,” said Dr. Zaba. “These chemotherapies only result in a durable response in approximately 5% of patients and so we typically reserve platinum-based chemotherapy only for palliation.”
Immune checkpoint inhibitors
“Whether Merkel cell is caused by polyomavirus or not, immune checkpoint inhibitors are extremely effective,” Dr. Zaba said. Prior to 2017, there were no treatments for Merkel cell carcinoma approved by the U.S. Food and Drug Administration (FDA). This all changed when the programmed death-ligand 1 (PD-L1) inhibitor avelumab was approved by the FDA and revolutionized the treatment of metastatic MCC.
Almost two years after the approval of avelumab, the PD-1 inhibitor, pembrolizumab, was approved for adults and children with metastatic or recurrent, locally advanced MCC. Both of these treatments have a similar response rate with about half of patients having persistent benefit for years, noted Dr. Nghiem, who serves as a consultant for Merck and EMD Serono. “For the other half — those who don’t persistently benefit — we’re working very hard through active trials and research to figure out how we can help these people.”
Single-agent immune checkpoint inhibitors, including PD-1/PD-L1 inhibitors, have a response rate of approximately 50-70% for first-line treatment of advanced stage III or stage IV Merkel cell carcinoma, Dr. Zaba said. “This high response rate to immune checkpoint inhibitors in patients with metastatic disease has resulted in the exploration of its use in high-risk locally or regionally advanced disease in several phase III adjuvant trials that are currently underway. The ADAM trial is investigating whether ICI can decrease MCC recurrence rate in stage III patients, and the STAMP trial is looking at decreasing recurrence in high-risk, completely resected stage I-III MCC patients.”
“It’s much more effective to use immune checkpoint inhibitors and to use it first,” Dr. Nghiem said, rather than starting patients with advanced MCC on chemotherapy first. “Those who have already received chemotherapy are significantly less likely to respond to subsequent immunotherapy. The chance of a response persisting is about 10 times higher for immunotherapy than chemotherapy,” he continued, “as long as it is given before chemotherapy.”
When a patient fails first-line immune checkpoint inhibitors, treatment becomes very tricky, Dr. Zaba noted. “There is nothing ‘curative’ for patients with advanced MCC that is not an immune checkpoint inhibitor, so we really drill down on that. Usually, we put the patient on a second immune checkpoint inhibitor — typically, adding a CTLA-4 inhibitor to PD-L1/PD-1 inhibitors.”
What the future holds
Other immune checkpoint inhibitors, including nivolumab (PD-1) and ipilimumab (CTLA-4), are also in clinical trials for the treatment of advanced MCC. In addition to immune checkpoint inhibitors, other forms of immunotherapy may also hold promise in the treatment of MCC, including cellular, intralesional, and single-fraction radiation therapy.
Approximately 50% of patients either do not respond to therapy or develop PD-L1 refractory disease and do not experience long-term benefit. Viral tumor antigens are a unique target of treatment, Dr. Park said. “A clinical trial of T-cell therapy targeting virus-specific antigens is ongoing, and a new trial of therapeutic vaccines to prevent recurrence is under development.”
“Several second-line agents for MCC are currently under investigation that continue to take advantage of the high immunogenicity of this tumor,” Dr. Zaba said. “The addition of the immune checkpoint inhibitor ipilimumab to PD-1 inhibitors can jumpstart the immune response in patients who are having disease progression on PD-1/PD-L1.”
For patients with locally advanced refractory skin disease, intralesional injection of talimogene laherparepvec (T-VEC) can be used, which is an oncolytic herpes virus that lyses the tumor and aids in immune cell maturation, Dr. Zaba explained. “Other second-line agents currently under investigation that can be used in combination with PD-L1 inhibitors include Lu-177DOTA-TATE in tumors expressing somatostatin receptors, and domatinostat, a histone deacetylase (HDAC) inhibitor, which is thought to increase the immunogenicity of MCC tumors.”
“Lu-177DOTA-TATE is a lutetium radioisotope hooked to oxodotreotide, which is the binding partner to somatostatin receptors which are highly expressed in about 50% of MCCs,” she said. “The Lu-177 is injected into the tumor, binds to the neuroendocrine cells, and kills them.” Some patients have highly expressing somatostatin receptor tumors and others do not, she added. “This treatment, which involves very expensive technology, is still under investigation.”
“For those patients who cannot tolerate immune checkpoint inhibitors, we can use the targeted therapy pazopanib, a multi-kinase inhibitor, to block upregulated tumor signaling pathways in MCC. This is similar to how we treat melanoma with a BRAF inhibitor combined with a MEK inhibitor for tumors that have a BRAF overactivation mutation,” she added, “although with Merkel, there isn’t an associated mutation, so pazopanib isn’t a miracle therapy, but it may prolong survival.”
A team effort
While effectively managing MCC is often a team effort, dermatologists are typically the physicians that will have found the lesion or will be consulting on the initial lesion, Dr. Nghiem said. “Dermatologists typically know more about Merkel cell carcinoma than physicians from any other field,” he continued. “I view the role of the dermatologist to be the traffic cop or orchestra conductor to stop any one field from going rogue. It’s human nature that the medical oncologist wants to infuse, a radiation oncologist wants to radiate, and a surgeon wants to cut. The dermatologist is really the patient’s advocate in this disease — from making the initial diagnosis, to following the patient for this cancer as well as other cancers over time.”
The MCC experts agree that dermatologists who encounter an MCC should order a PET-CT scan and ensure rapid referral to surgery and radiation. “Bottom line: If you don’t care for Merkel cell patients all the time, take care of your patient, but don’t be the only one,” Dr. Nghiem said. “It needs to be a team effort and dermatologists shouldn’t be afraid to advocate on behalf of their patients. And, usually, that means getting multidisciplinary expertise early. You need multidisciplinary care, and you need updated information because things are changing really fast.”

{kind=link}